Article Text

Abstract
Terrorist events in the form of explosive devices have occurred and remain a threat currently to the population and the infrastructure of many nations worldwide. Injuries occur from a combination of a blast wave, energised fragments, blunt trauma and burns. The relative preponderance of each injury mechanism is dependent on the type of device, distance to targets, population density and the surrounding environment, such as an enclosed space, to name but a few. One method of primary prevention of such injuries is by modification of the environment in which the explosion occurs, such as modifying population density and the design of enclosed spaces. The Human Injury Predictor (HIP) tool is a computational model which was developed to predict the pattern of injuries following an explosion with the goal to inform national injury prevention strategies from terrorist attacks. HIP currently uses algorithms to predict the effects from primary and secondary blast and allows the geometry of buildings to be incorporated. It has been validated using clinical data from the ‘7/7’ terrorist attacks in London and the 2017 Manchester Arena terrorist event. Although the tool can be used readily, it will benefit from further development to refine injury representation, validate injury scoring and enable the prediction of triage states. The tool can assist both in the design of future buildings and methods of transport, as well as the situation of critical emergency services required in the response following a terrorist explosive event. The aim of this paper is to describe the HIP tool in its current version and provide a roadmap for optimising its utility in the future for the protection of national infrastructure and the population.
- trauma management
- oral & maxillofacial surgery
- preventive medicine
Data availability statement
Data sharing not applicable as no datasets generated and/or analysed for this study. This is a review article.
Statistics from Altmetric.com
Key messages
The Human Injury Predictor tool is a computational model which was developed to predict the pattern of injuries following an explosion.
Validation of the tool was determined using clinical data from the ‘7/7’ terrorist attacks in London and the 2017 Manchester Arena terrorist event.
The tool currently is used to assist both in the design of buildings and methods of transport such as underground trains.
Future iterations of the tool will aim to predict the number and location of critical emergency services required in the response following a terrorist explosive event.
Introduction
Terrorist events are a threat to both the population and the infrastructure of many nations worldwide. The terrorist threat we currently face is multifaceted, diverse and continually evolving.1 Terrorist events have most commonly used improvised explosive devices (IEDs)2 and marauding individuals with blades.3 4 The two defining terrorist events in the UK that have used explosive devices in the 21st century were the ‘7/7’ bombings in London in 20055 and the Manchester Arena bombing in May 2017.6 An IED placed at Parsons Green underground station later in 2017 failed to initiate properly, potentially preventing numerous fatalities. Injuries from these IEDs occur from one or more mechanisms, which are commonly classified into primary to quinary, occurring from a combination of a blast wave, energised fragments that are carried by the blast wind, blunt trauma and burns.7 The relative preponderance of each injury mechanism is dependent on the type of device, distance to targets, population density and the surrounding environment, such as occurring in an enclosed space, to name but a few.
Government policy
The first duty of the government is to protect the public, and the police, security services and other partners do all they can to combat the threat of terrorist attacks: since March 2017, in the UK alone 27 terrorist plots have been foiled. However, organisations must be empowered to do more. The Protect Duty consultation was run by the UK government between February and July 2021.1 It sought views on how legislation could be used to enhance the protection and safety of public spaces and other publicly accessible locations. The proposed legislation from this consultation came primarily from the reaction to the Manchester Arena bombing, particularly the campaign to introduce ‘Martyn’s Law’, named after 29-year-old Martyn Hett, who was tragically killed in the Arena bombing.8 The aim of the Protect Duty would be to impose a legal obligation on organisations to consider the safety of their staff and the public who use their facilities from threats such as terrorist events.
Optimisation of infrastructure to reduce injuries from explosive events
Using lessons learnt often from the battlefield, medical treatment of casualties from blast injury in the civilian setting has reached unprecedented levels of efficacy from the point of wounding and beyond; in the military this has resulted in an increased number of survivors even with severe wounds,9 although the degree to which this can realistically occur in the national health service must be questioned. Survivability from explosive events in the military environment can be improved through primary prevention, mainly using armour worn by individuals or incorporated into vehicles. In the civilian environment, survivability can alternatively still potentially be increased through optimisation of infrastructure. This comprises multiple interventions, including the design of buildings, the distribution density and location of the population at risk, and the location of emergency responders (Table 1).
Potential methods to optimise infrastructure to reduce the number and severity of casualties from explosive events in the civilian setting
Modelling of injury from explosive events
When attempting to estimate the clinical effects from explosive events, two broad categories of injury models are generally used.10 Additionally, some predictive information can be gained from studying the epidemiology of previous terrorist events.2 The first type of injury model, and still the most common, is physical models, which encompass animal surrogates and inert simulants such as gelatine.11 The second category is numerical models, in which computer simulations are used to represent the weapon–target interaction. Although numerical models overcome many of the limitations in using animals or simulants, such as ethics and cost, the mathematical algorithms that underpin their predictions still require the output from physical models to inform and validate them. Examples of injury modelling include those of ballistic threats,12 behind armour blunt trauma,13 trauma due to primary blast14 and vehicle occupant injury when a vehicle is attacked by an explosive threat; the main goal of these models has been to inform strategy on mitigation through personal protective equipment, infrastructure and vehicle design, or behaviour.
Development of the Human Injury Predictor tool
The Human Injury Predictor (HIP) is a numerical model developed to simulate the primary and secondary (penetrative fragmentation) blast effects of a detonation of an IED within crowds of people in metropolitan environments.5 HIP was developed in the UK by the Defence Science and Technology Laboratory in conjunction with the Centre for the Protection of National Infrastructure. The HIP code was originally developed to assist in the coroner’s inquests into the 7 July 2005 London terrorist bombings.5 Clinicians from the Royal Centre for Defence Medicine had advised on clinical parameters for HIP, based on experience gained in regular reviews of operational mortality for UK service personnel injured in Iraq and Afghanistan.15 Since then, HIP has been used successfully to identify potential risks to infrastructure projects, including those for the London 2012 Olympic Games.
How HIP currently models blast injury in an urban environment
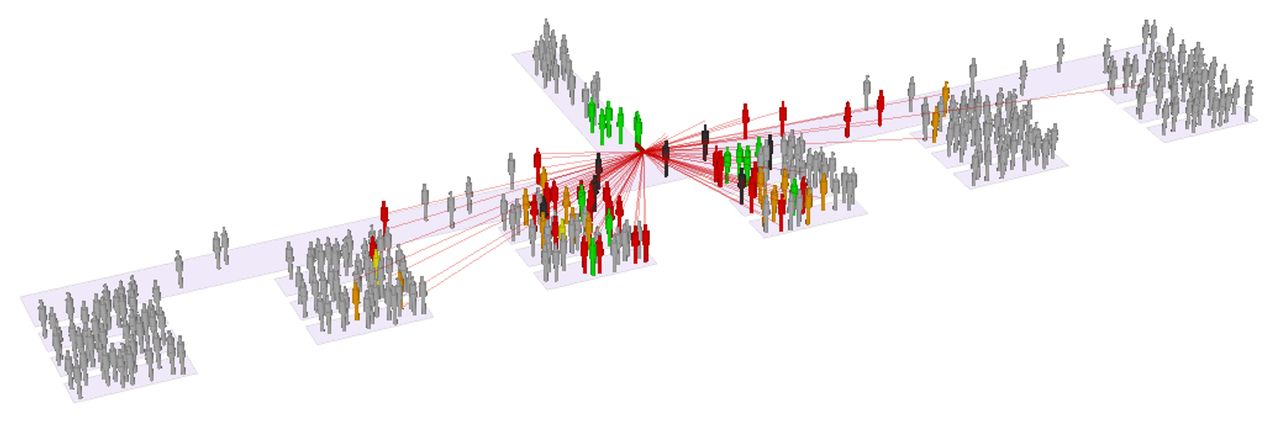
Within HIP, a number of broad variables are modelled, including an explosive device, humans within a crowd and the environment (Figure 1). These variables can be modified to simulate a family of scenarios of interest. HIP simplifies the body into five cylinders, each representing one body area (head, neck, chest, abdomen and legs), and can distribute people randomly within user-defined areas and density. It can distribute fragments randomly within defined patterns and simulate different sizes of explosive. The building architecture can be customised by defining floors and obstacles, such as walls, rooms and stairs/grandstands. All obstacles can be set to be impermeable to fragments, or have a defined penetration capability. Only closed rooms are currently used to simulate blast wave reflections; other obstacles do not offer any shielding or reflective effects. In additions, stairs/grandstands can be designated as having a population so that people using stairs or stadiums can be simulated. HIP does not include penetrating wounds from the shattered glass of windows as the vast majority of work on glazing revolves around hazard levels based on where the fragments go; the link to what the fragments actually do to people is not currently known in any detail.

HIP simulation being used to provide a graphical representation of the effects of an explosive device detonated within a queuing crowd. HIP, Human Injury Predictor.
HIP is currently capable of estimating severity of injury due to both primary and secondary (penetrating fragment) aspects of blast. The manner in which HIP represents primary blast is dependent on the environment, with open air detonations using a free-field ‘Friedlander’ type of temporal displacement, whereas those in enclosed environments use a superposition method derived from hydrocode runs to determine pressure and impulse loading.5 Primary blast injury is determined for the head, chest and legs. For the head, a simple threshold pressure level is used to determine eardrum rupture, with an Abbreviated Injury Scale (AIS) score of 1 used if eardrum rupture is predicted. The primary blast injury to the chest is based on the lethality probability from Bowen curves,16 with levels mapped to AIS scores. The primary blast injury to the leg is determined by a threshold pressure-impulse level which correlates to a likelihood of traumatic amputation, with an AIS score of 6 if traumatic amputation is predicted.
Fragmentation penetration due to secondary blast is based on algorithms depicting depth of penetration (DoP) of a range of fragments into 20% gelatine, demonstrated to represent the muscle accurately.10 The DoP into each cylinder produces an injury score for that body region, based on extrapolation of the methodology used in the AIS system. The highest three scores from both primary and secondary injury are squared and summed to produce an overall severity score (with the exception being that if the AIS score is 6, the score is automatically 75), in an approach designed to be analogous to the manner in which a New Injury Severity Score is calculated.
Validation of the HIP code
Analysis of the Manchester Arena bombing was the first time in which the code, specifically developed from data from 7/7, could potentially be validated to a real-life event. This event was different from 7/7 in that it occurred in a relatively large open space (unlike an underground train or bus) and the IED was of different design in both the explosive used and the preformed fragments embedded around it. Due to the ongoing public enquiry, only the clinical records of survivors can currently be analysed and the report itself must remain restricted until the enquiry is complete.17
Clinical data for all 140 survivors were analysed using the Trauma Audit Research Network database supplemented by clinical records. Clinical findings were compared with those predicted by the secondary blast component of HIP using a set-up of building architecture and crowd distribution similar to the incident. Clinical records suggest that injuries due to secondary blast predominated (76% of injuries), followed by tertiary (24%) and quaternary (7%). No evidence for primary blast injuries in survivors of the terrorist event was found. Multiple scenarios were run using the existing baseline (ie, that derived from the 7/7 bombings) and additional permutations in terms of fragment numbers and initial velocities until an HIP scenario was produced that closely matched the clinical findings. This required an increase in predicted fragment initial velocity and number from that of the existing baseline.
To parameterise and validate the weapons effects algorithms within the HIP, controlled physical testing has been used to study the behaviour of ejected fragments.5 Explosives were initiated within a test arena that contained arrays of water-filled cylinders to represent crowds of humans; fragment trajectories and target interactions were quantified using high-speed video diagnostics. Separate experiments involving individual fragments projected from gas guns, quantified projectile penetration into various materials and flash X-ray were employed to look at the spatial distribution of fragments during the very early stages of ejection. Standard diaphragm-based transducers were also used to measure pressure-time histories in the far-field and near-field blast environments (Figure 2).18

Schematic of the CoBL apparatus (not to scale): (A) elevation; (B) detailed plan view of the target plate showing bar arrangement and coordinate axes (adapted from O'Connell et al 19); and (C) comparison of numerical and experimental peak-specific impulse distributions for 100 g PE4 sphere at 55.4 mm clear stand-off distance (adapted from Axelsson and Yelverton20). CoBL, characterisation of blast loading.
Suggested future direction of the HIP code
There is a drive to refine how scores are currently assigned within HIP to reflect better the predicted penetration and blast injury as part of a generalised approach to improvements in injury modelling. These can be defined broadly as improvements to five components: the weapon, the target, the clinical effect, the proposed response and the user interface. It is this last parameter that is essential to enable planning of the siting of emergency responders and thereby ensure a coordinated multidisciplinary response.
Weapons effect representation
HIP currently models primary and secondary blast only, but with the desire to include tertiary and quaternary blast. Tertiary blast, by which energised casualties collide with objects or structures, predominantly causes blunt trauma; however, each individual scenario is incredibly hard to model, such as predicting the strength of the blast wave required to displace a victim, the victim’s velocity on subsequent impact with an object, and finally the location of impact both on the victim and the object itself. Tertiary blast alone is rarely lethal, and due to the complex computational power required to model them there is understandably less impetus to model these injuries currently. Thermal injury (quaternary blast) includes both surface burns and inhalation injury; although clinically important when they occur, thermal injury and its sequelae generally have a relatively low incidence in immediate survivors from blast injury and will not be modelled currently.
Target representation
The current division of the human body into five body areas is efficient computationally but remains a gross simplification. Increased fidelity in representing the human body could be achieved by dividing the body into a greater number of subsections, such as separating the arms from the legs, and the face from the head, as in the AIS methodology. This would enable comparisons with clinical outcome data from military blast casualties described in the Joint Theatre Trauma Registry, which uses AIS as part of the injury descriptors.19 Ideally, each human would instead be represented as an anatomically correct structure, such as is used in higher fidelity models used within the government, such as the Coverage of Armour Tool used to compare personal armour designs,12 and include the vital organs. Additionally, different sizes of target (ie, anthropometry) would also be available, reflecting that sadly many of those injured in these events have been children.
Clinical effect
Primary blast injury
The prediction of primary blast injury is complex. Empirical methods exist that can estimate the levels of human injury in the free field (such as the Bowen curves currently implemented in HIP), but there are no mature methods that can quickly predict complex blast propagation in enclosed environments or simulate the associated physical disruption. Many areas that are susceptible to explosions are enclosed and so a method is required that can take inputs from a complex blast pressure history and produce the associated human response and link to an injury outcome. A prototype version of the single degree of freedom (SDOF) Axelsson and Yelverton method for predicting chest wall response to primary blast20 is currently being trialled in HIP to test whether injury outcome prediction is improved. In addition to the chest wall SDOF model, other single and multiple degree of freedom models are required to represent primary blast response of other areas, such as the legs and the abdomen; however, the chest remains the first priority as it is the injury that dominates mortality at the lowest pressure/impulse levels.
Secondary blast injury
Currently, it is the DoP of a fragment into a body area (which is represented on algorithms based on 20% gelatine) that is used to determine the severity of injury and assign an injury score. Such an approach is recognised to be overly simplistic. Newer evidence from military injuries exists to relate the minimum DoP from skin to critical anatomical structures in each body area21 and injury-risk curves now exist that can relate a metric in the projectile (such as impact velocity) with injury severity.22 In addition, projectile directionality, with entry points to the front and rear as an absolute minimum, should be included; without this, the predicted penetration depth causing a particular injury must be averaged around the whole circumference of that body area.
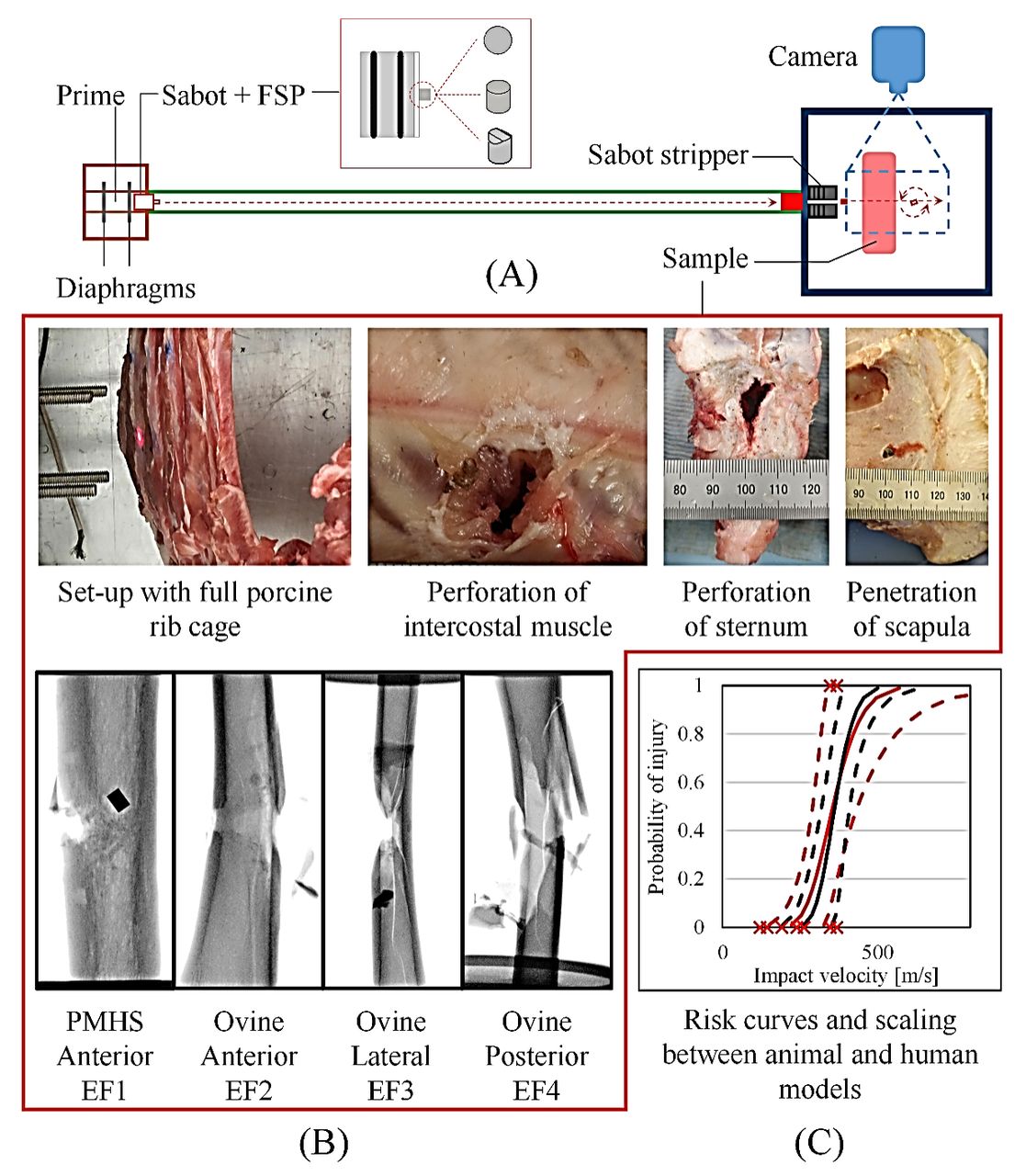
Outputs from experimental studies are necessary to improve the accuracy of, and test for validation, the injury outcome predicted by computational models. Experimental data can be used to advise on (1) the penetration threshold of various tissues and organs, (2) the severity of injury as a function of an input variable such as projectile impact velocity, and (3) the residual velocity and behaviour of the projectile after the impact. Recently, ballistic tests (Figure 3), using a gas-gun system with different projectiles, were performed on multiple bone structures and organs such as the tibia, rib bone, scapula, sternum, muscle and heart.23–27 In these studies, statistical survival analysis was carried out to obtain the risk for a specific severity of injury outcome and the effects of direction and location of the impact on injury outcome were investigated.

{kind=link}
{kind=link}
{kind=link}
(A) Experimental set-up using the gas-gun system and different metal projectiles for testing various tissues and organs. (B) Examples of samples studied: the penetration and perforation of various porcine thoracic tissues (ribs, sternum, scapula and intercostal muscle); and the ovine specimen and postmortem human specimen (PMHS) used in directional mapping of the tibia fracture rated to the modified Winquist-Hansen classification (Extraarticular Fracture Types 1-4, EF1–EF4, fracture patterns). (C) Resultant injury-risk curve, relating the probability of an injury outcome to the level of threat, was obtained with the animal model and scaled to the relevant human model. FSP= Fragment Simulating Projectile.
Proposed emergency response
The use of injury scores is helpful when making comparisons between different parameters, such as charge size and population density; however, it has limited utility for those responsible for medical planning, such as the emergency medical services (EMS). Instead, it is recommended that the model also predicts triage states, which are used to convey the urgency of treatment and enable prioritisation to those who need it most. This could be based on the National Ambulance and Resilience Unit Triage Sieve, which is used by EMS in the UK,28 adapted from the UK military’s former Major Incident Medical Management and Support (MIMMS) Triage Sieve.29
Functionality
To enable maximum utility by those responsible for emergency preparedness, HIP must have a simplistic end-user interface. The sheer computing power required for the calculations means that predictions are completed within timeframes unlikely to be useful for an acute response to an incident. Instead, the code’s utility lies in the planning of predicted scenarios and the design of infrastructure and events.
Conclusions
HIP has already demonstrated its utility to those responsible for planning infrastructure in predicting the clinical effects of a terrorist explosion. Analysis of the injuries sustained by the survivors of the Manchester Arena bombing demonstrated a correlation between the injuries predicted and those seen clinically. However, further work is required to validate the tool’s utility for different charge sizes and population densities. The fidelity of its predictions will be improved by subdivision towards greater numbers of body areas, penetration directionality and incorporation of DoP into known critical anatomical structures. Further development of the tool should focus on the end-user interface and the generation of triage scores to enable the EMS to allocate medical resources optimally. Mature tools such as HIP can help government departments and individual organisations achieve improved primary injury prevention and survivability of the population from terrorist attacks in nations worldwide.
Data availability statement
Data sharing not applicable as no datasets generated and/or analysed for this study. This is a review article.
Ethics statements
Patient consent for publication
Ethics approval
This study does not involve human participants.
Acknowledgments
Part of this work was conducted at the Royal British Legion Centre for Blast Injury Studies at Imperial College London; therefore, the financial support of the Royal British Legion is gratefully acknowledged.
References
Footnotes
Twitter @icsmas
Contributors JB: review, drafting, final approval of the manuscript, overall responsibility. RNF, T-TNN, AR, DP, SDM: review, drafting, final approval of the manuscript.
Funding This work received financial support from the Royal British Legion.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.