Article Text

Abstract
Introduction Haemorrhage is the leading cause of potentially survivable death on the battlefield. Despite overall improvement in battlefield mortality, there has been no improvement in survival following non-compressible torso haemorrhage (NCTH). The abdominal aortic junctional tourniquet-stabilised (AAJT-S) is a potential solution that may address this gap in improving combat mortality. This systematic review examines the evidence base for the safety and utility of the AAJT-S for prehospital haemorrhage control in the combat setting.
Methods A systematic search of MEDLINE, Cumulated Index to Nursing and Allied Health Literature and Embase (inception to February 2022) was performed using exhaustive terms, in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guideline. The search was limited to English-language publications in peer-reviewed journals; grey literature was not included. Human, animal and experimental studies were included. Papers were reviewed by all authors to determine inclusion. Each study was assessed for level of evidence and bias.
Results 14 studies met the inclusion criteria: 7 controlled swine studies (total n=166), 5 healthy human volunteer cases series (total n=251), 1 human case report and 1 mannikin study. The AAJT-S was demonstrated to be effective at cessation of blood flow when tolerated in healthy human and animal studies. It was easy to apply by minimally trained individuals. Complications were observed in animal studies, most frequently ischaemia-reperfusion injury, which was dependent on application duration. There were no randomised controlled trials, and the overall evidence base supporting the AAJT-S was low.
Conclusions There are limited data of safety and effectiveness of the AAJT-S. However, there is a requirement for a far-forward solution to improve NCTH outcomes, the AAJT-S is an attractive option and high-quality evidence is unlikely to be reported in the near future. Therefore, if this is implemented into clinical practice without a solid evidence base it will need a robust governance and surveillance process, similar to resuscitative endovascular balloon occlusion of the aorta, with regular audit of use.
- accident & emergency medicine
- trauma management
- surgery
Data availability statement
No data are available.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Non-compressible torso haemorrhage (NCTH) is the leading cause of potentially survivable battlefield death.
There has been no improvement in the mortality rate from NCTH in the last two decades, despite a significant overall improvement in mortality rate.
NCTH deaths are predominantly early, and therefore any interventions should have far-forward utility.
WHAT THIS STUDY ADDS
This study summarises the literature for the abdominal aortic junctional tourniquet-stabilised (AAJT-S).
There is limited evidence of the safety and effectiveness of the AAJT-S.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
A far-forward NCTH solution is required, and further evidence is unlikely to be forthcoming in the near future.
Currently, the only viable solution for far-forward use is the AAJT-S.
If this is implemented into clinical practice without a solid evidence base it will require a robust governance and surveillance process, similar to resuscitative endovascular balloon occlusion of the aorta, with regular audit of use.
Introduction
Haemorrhage is the leading cause of potentially survivable death on the battlefield.1 2 US military data have demonstrated an 85% reduction in mortality of extremity haemorrhage following the adoption of arterial limb tourniquets.1 The remaining challenges in improving haemorrhagic trauma survival are therefore focused on torso (chest, abdomen, pelvis) and junctional (axilla, groin) haemorrhage.3 In potentially survivable combat trauma, the prevalence of torso haemorrhage death is 3.5 times that of junctional haemorrhage,2 and in some treatment situations junctional (particularly groin) haemorrhage is considered torso. The term NCTH has been coined to describe significant haemorrhagic injury in the torso,4 and presents the greatest opportunity to improve combat trauma survival.3
The NCTH combat fatality rate of UK personnel during the first decade of Op HERRICK (Afghanistan, 2002–2014) was 86%, and 88% of these casualties died prehospital.5 While there was a year-on-year improvement in the case fatality rate,6 significant improvement in mortality from extremity haemorrhage and severe injury,7 temporal analysis has demonstrated no significant improvement in NCTH survival during Op HERRICK.5 In casualties who died prehospital with torso and proximal lower limb trauma, the median time to death (excluding immediate deaths) was 29 min.6 This suggests that a solution is needed, and that this solution should be simple enough to be used prehospital, ideally at the point of wounding. The best intervention would have the following military requirements: to be applied close to point of wounding, prevent exsanguination and have the potential of utility in prolonged field care without undue iatrogenic complications. While the prehospital use of resuscitative endovascular balloon occlusion of the aorta (REBOA), and resuscitative thoracotomy have been reported in the civilian setting,8 9 these advanced interventions are unlikely to be delivered far-forward, let alone within a few minutes at the point of wounding by non-medical personnel in a combat setting. Intra-abdominal foam/sealants have likewise been suggested as a potential solution,10 but these need further development, an evidence base and demonstrated suitability for use far-forward.
The AAJT-S is an external compression device, placed around the abdomen with the aim of occluding the aorta.11 It was approved as a class II medical device by the US Food and Drug Administration in 2023 (a previous version, the AAJT, was approved in 2013), and can potentially provide rapid infrarenal vascular control of pelvic, junctional groin/buttock and very proximal lower limb haemorrhage not amenable to arterial tourniquet control.11–13 The AAJT-S can be used by trained non-medical personnel, requires no maintenance, is small and lightweight and can be applied to a conscious patient. The anatomical site of haemorrhage control means that the AAJT-S is not a complete NCTH solution. However, its simplicity provides an attractive potential option on multiple levels to a proportion of combat NCTH cases. There have been a number of studies of the AAJT-S, but these data have not been synthesised. The aim of this systematic review was to report the existing evidence base for the safety and utility of the AAJT for prehospital haemorrhage control in the combat setting.
Methods
Protocol and registration
This systematic review uses the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guideline,14 and has been registered in the international prospective register of systematic reviews (awaiting PROSPERO number).15
Search strategy
A systematic search of MEDLINE, Cumulated Index to Nursing and Allied Health Literature and Embase from inception to February 2022 was performed by a trained librarian using exhaustive terms, in accordance with the PRISMA statement.14 The inclusion criteria were: human, animal, mannikin subjects; controlled studies and case series/reports, which reported novel safety and/or effectiveness data relevant to traumatic haemorrhage. Search terms included: torso; haemorrhage; haemorrhage; abdominal; tourniquet, and was limited to English-language publications in peer-reviewed journals (online supplemental table 1). Grey literature was not included.
Supplemental material
Study selection
Abstracts were independently screened, duplicates removed and full papers subsequently reviewed by all authors to identify whether a study met the inclusion criteria. Full paper references were screened to identify any additional studies not previously screened; these were also reviewed by all authors to determine inclusion. Arbitration was by the senior author. Outcome measures included in the analysis were: successful occlusion of blood flow, time of application, clinical effectiveness, clinical safety or complications found and ease of use.
Risk of bias, and levels of evidence assessment
Each study underwent an assessment of bias using the ROBINS-I (Risk Of Bias In Non-randomised Studies - of Intervention) tool,16 and was evaluated for level of evidence (centre for evidence-based medicine).17 Data on type of study, subject type, comparison groups, number of participants and outcome measures including effectiveness in haemorrhage control, and safety were collated in a Microsoft Excel data sheet.
Results
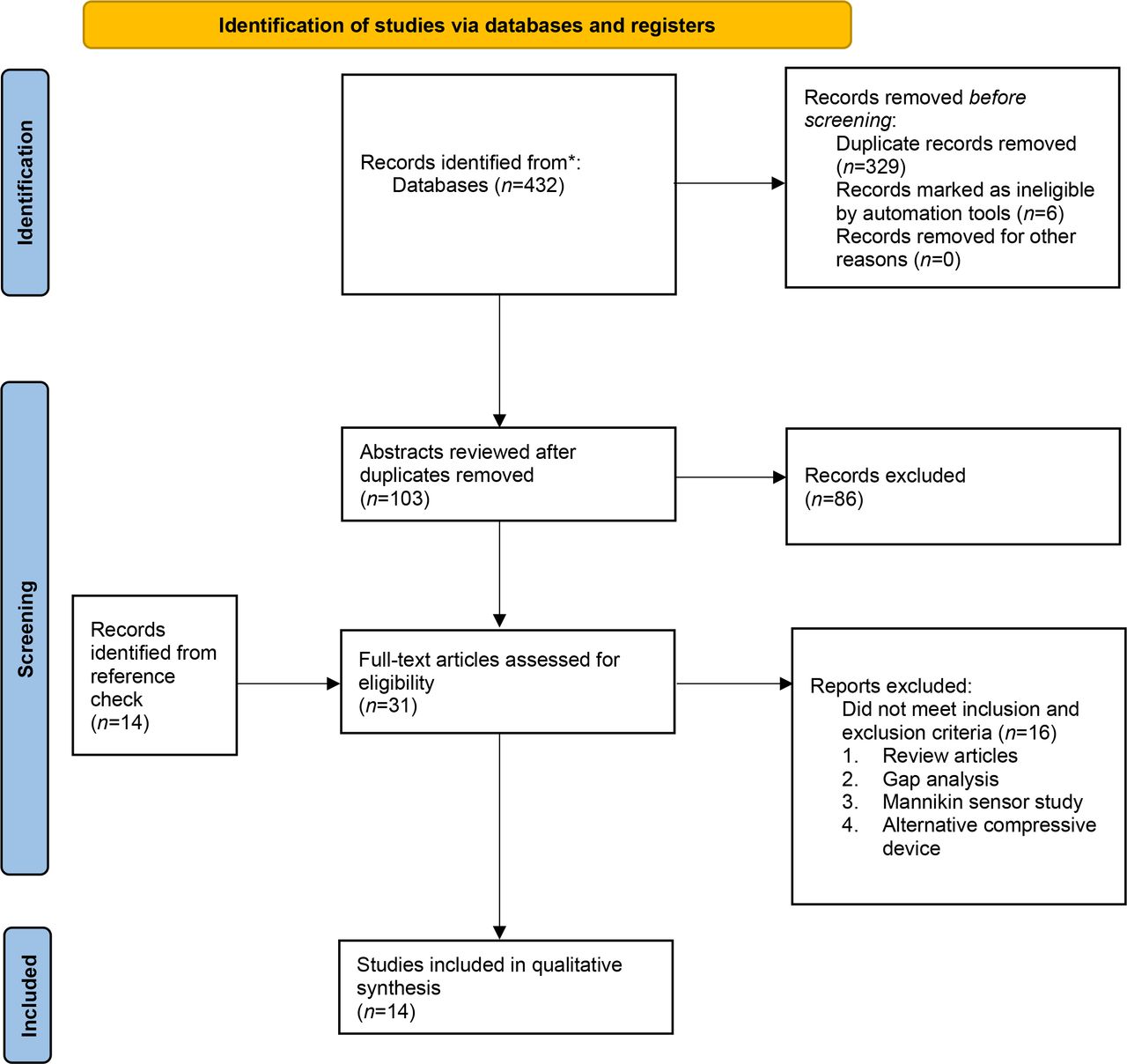
A total of 14 studies met the inclusion criteria (Figure 1). These papers included: seven controlled swine studies (total n=166), five healthy human volunteer cases series (total n=251), one mannikin study and one human case report.

Abdominal aortic junctional tourniquet-stabilised systematic review Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram.
Animal studies
There were n=7 (50%) animal studies (Table 1). All studies were small preclinical animal (swine) case series. Meta-analysis was not appropriate due to methodological heterogeneity. The AAJT-S was reported to occlude distal flow in traumatically injured swine in three studies (n=72), and control bleeding in three studies (n=70) compared with controls. One study reported no occlusion of flow. However, the AAJT-S was only inflated to a pressure of 40 mm Hg for an application time of 10 min.18 When compared with ‘no treatment’, mortality benefits were observed in all cases for the duration of the study. When compared with alternative treatments such as fluid therapy, open peritoneal packing or REBOA, a mortality benefit was seen in two out of six studies. Mean arterial pressure (MAP) was reported to increase immediately following AAJT-S application by 70 mm Hg,13 a statistically significant increase in systemic vascular resistance (afterload) was also observed.12
Abdominal aortic junctional tourniquet-stabilised systematic review animal studies
Complications
The most frequently reported complication was ischaemia-reperfusion injury, which occurred when the AAJT-S was released and lead to metabolic derangements (hyperkalaemia, hyperlactataemia, metabolic acidosis); there was no significant difference in lactataemia between AAJT-S and REBOA. This suggests that (lactate) is dependent on aortic flow (rather than tissue compression).19 Compression occurring inferior to the renal vessels did not affect renal perfusion.20
Compression-related complications were observed in three studies including: bladder/bowel pressure necrosis in 50% of swine,21 hydronephrosis (ureteric compression) and small bowel necrosis in applications of 240 min,20 irreversible splanchnic nerve injury and hind leg paraplegia in applications >60 min.22 One study reported that 3 out of 12 swine had vena caval thrombus. However, 2 out of 12 of the control swine also had a vena caval thrombus.18 Therefore, this may not be a complication of the AAJT-S, and instead a sequela of hypovolaemia and high-volume blood resuscitation. Other studies demonstrated no complications following a 120 min AAJT-S application in swine.12 Overall, complications appeared to be more prevalent in longer-duration applications. Consensus was that a 60 min application time was considered to be safe without irreversible complications.19 20 22
Human and mannikin studies
All five healthy volunteer studies (n=251 applications) included male-only participants (Table 2). These studies demonstrated that the AAJT-S was quick and easy to apply with minimal training, and had high user satisfaction scores.23–25 Mean application times were reported between 60 and 75 s in daylight and low light settings.24 A mannikin model comparison of AAJT-S and other compression devices (Combat Ready Clamp CRoC, Junctional Emergency Treatment Tool and SAM Junctional Tourniquet) reported that AAJT-S had the greatest effectiveness, and second-fastest application time.26 This study also reported high rates of AAJT-S bladder failure when used repeatedly, confirming that this is indeed a single-use device.26
AAJT-S healthy volunteer and mannikin studies
Methodology differed between the studies, but some themes were consistent. Application time ranged from immediate removal on cessation of flow to up to 60 s. Cessation of flow was demonstrated by use of arterial Doppler in all studies. The success rate of the AAJT-S in occluding aortic blood flow demonstrated significant variation, owing to subject pain before the recommended AAJT-S bladder pressure could be achieved. The greatest reported success rate was 94%,25 whereas the lowest was only 11%, owing to pain.27 Two out of five studies reported pain to be significant, allowing occlusion in <30% of applications. British studies had a higher success rate 84% (42/50),24 25 compared with US studies 30% (17/57); the average for all studies was 55% (59/107). In the studies that reported a pain score, the mean score was 7/10 (n=55). It is hypothesised that in critically injured bleeding trauma patients this would not be an issue.28 Pain was the only reported complication. Triphasic flow was found to return in participants after 1 min. One study followed up volunteers after 2 weeks and no complications were reported.
Case report
The single case report of AAJT-S use was from the USA in Afghanistan (2013). The device was used successfully in traumatic cardiac arrest secondary to high bilateral lower limb amputations that were not amenable to arterial tourniquets. An immediate increase in end-tidal carbon dioxide was observed together with the return of a palpable carotid pulse. At 48 hours, the patient was noted to have no signs of bowel ischaemia or renal failure.29 However, the duration of AAJT-S application was not reported.
Levels of evidence
Animal studies and healthy human volunteer studies are designed to test safety and effectiveness of new treatments, and devices cannot be assigned a level of evidence. Therefore, the only published AAJT-S data that can be applied is the single case report; level 5 (mechanism-based reasoning).17
Bias assessment
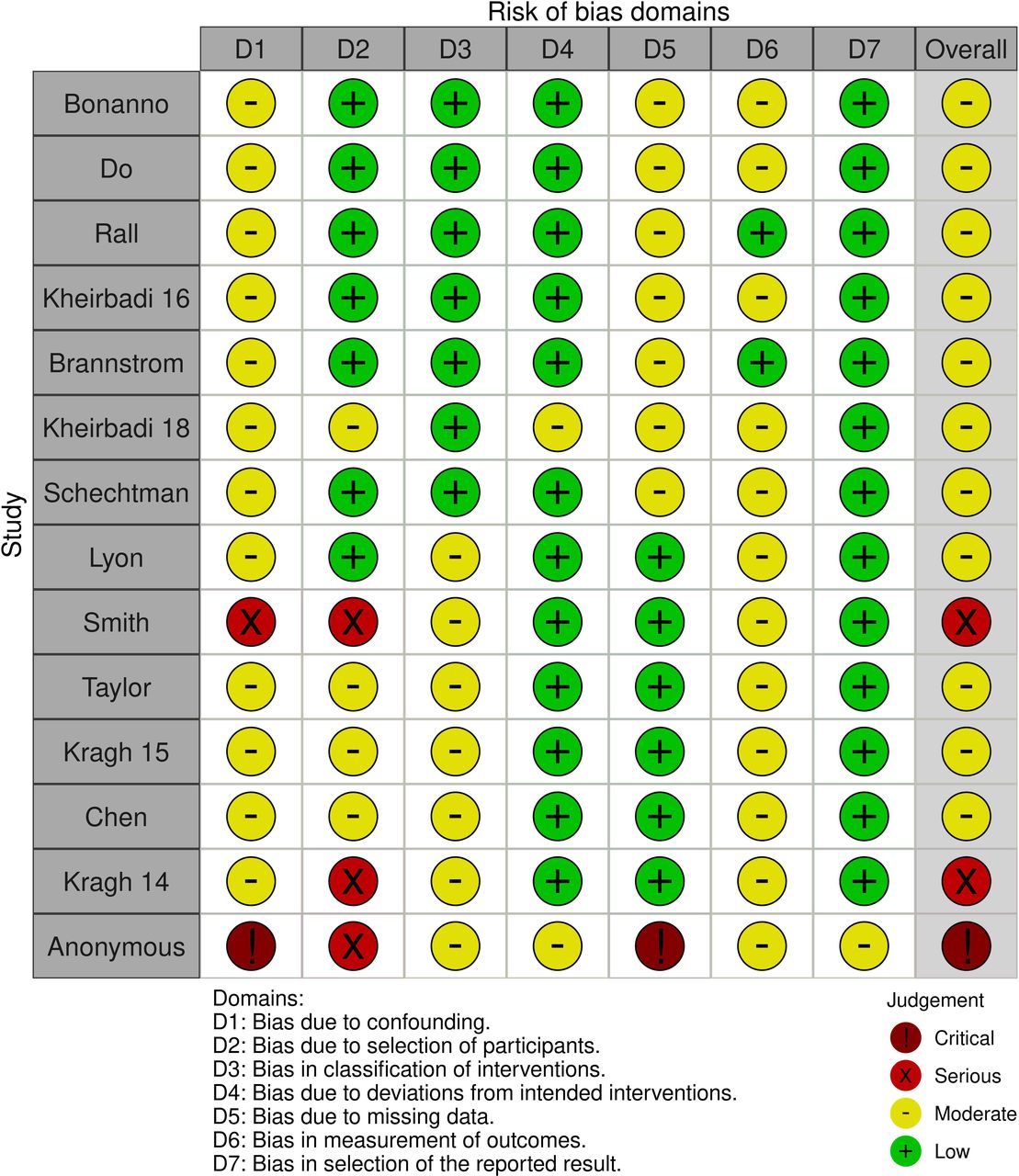
Most studies were found to be at moderate risk of bias overall (ROBINS-I tool).30 Two studies had serious risk, and one had critical risk of bias. The confounding domain was found to be the most influential in the overall assessment (Figure 2).

Abdominal Aortic Junctional Tourniquet - Stabilised (AAJT-S) systematic review bias assessment using Risk Of Bias In Non-randomised Studies - of Interventions (ROBINS-I) tool.
Synthesis of findings across all published studies
The AAJT-S has been demonstrated to be effective at cessation of flow when tolerated in both healthy human and animal studies (Figure 3). It is easy to apply by minimally trained individuals in ≤90s, and this application time has been reported to be replicable in a variety of settings. No long-lasting complications were seen in healthy human volunteer studies, pain was found to be the most significant complication in the studies resulting in incomplete occlusion; pain resolved on removal of the device. Complications were observed in the animal studies, most commonly ischaemia-reperfusion injury, and this was dependent on application duration. Although there was some variability seen across the studies, consensus was that safe application time should not exceed 60 min. There are no randomised controlled trials, and the overall evidence-base supporting the AAJT-S is low.

{kind=link}
{kind=link}
{kind=link}
Abdominal Aortic Junctional Tourniquet - Stabilised (AAJT-S). Photograph courtesy of Compression Works LLC, Birmingham, AL, USA.
Discussion
The AAJT-S is quick and easy to apply, and effectively occludes aortic flow distal to the renal vessels in animal models and healthy human volunteers. A single case report of successful AAJT-S use provides limited assurance of real-world utility in the combat setting. The incidence of complications varied between studies, but overall, there is signal that increased durations of occlusion are associated with greater risks, and a consensus that AAJT-S application should not exceed 60 min. The level of evidence is low, and prospectively identifying patients who may benefit is very challenging. However, there is a well-defined need for far-forward interventions to reduce mortality in NCTH, and the AAJT-S is a potential solution.
Patient selection
One of the key attributes of the AAJT-S is that it can be successfully applied with minimal training.24 Those who die from NCTH due to battlefield trauma do so quickly,6 and therefore any future intervention to improve mortality in this patient group must be within the scope of practice of those close to point of injury. The AAJT-S is indicated for haemorrhage distal to the infrarenal vessels, controlling bleeding in the pelvis, inguinal region and lower extremities.31 A REBOA gap-analysis of UK combat casualties demonstrated that in those with injuries amenable to zone 3 REBOA (a similar indication to AAJT-S), >40% may have benefited.32
Patient selection is likely to be fundamental to effective use of the AAJT-S. The current issue is that there is no consensus of who will die without prehospital NCTH interventions (REBOA, intra-abdominal foam, AAJT-S, etc), and who will survive without it, and thereby avoid iatrogenic harms. Furthermore, we do not have clear evidence that the AAJT-S (or REBOA) is of overall benefit to any patients. Unless we can identify a cohort who will benefit, we cannot set inclusion criteria for a trial to test the hypothesis of benefit, and without the ability to test the hypothesis we cannot be sure if this cohort even exists, and if it does how to identify them. While the AAJT-S is likely to carry significantly less risk than REBOA, its main strength is the ability to deploy far-forward where the greatest impact is likely to be. One proposition for reducing iatrogenic harms from REBOA is for partial or intermittent occlusion. There is no evidence that this is possible with the AAJT-S, and indeed partial occlusion may simply cause venous congestion and increased venous bleeding. This is a complex area of high-level decision-making with very limited evidence, and therefore at the current time a consensus-based recommendation for clinical practice is the only realistic outcome of this review. The only practical direction is implementation alongside a robust governance system that allows rapid identification of potential harms.
Prolonged field care
Currently, the war in Ukraine is forcing us to again consider the implications of war fighting at scale. The literature has shown that in animal studies while the AAJT-S can be applied to spontaneously ventilated injured swine, to prevent respiratory arrest in all cases they must be mechanically ventilated prior to removal.13 Translating this to the military setting would mean that while the device could be applied by medics close to the point of injury it may need to be removed at role 2.
Complications were broadly proportional to the duration of AAJT-S application.20 22 In the healthy volunteer studies, application time was very short and no complications were seen, other than pain during application. Tissue ischaemia was the most frequently reported complication rather than compressive forces, which is supported by the similar side-effect profile and lactate recorded in the study by Schechtman et al comparing AAJT with REBOA.19 In the animal studies, complications seen after 1 hour of application were reversible, in comparison to those seen after 2 hours: acidaemia, spastic paraplegia, muscle necrosis and bladder/bowel dysfunction.22 When considering the safe application time for other aortic occlusion devices 60 min is also often quoted as the time before significant ischaemic injury begins to occur.33 This may limit the utility of the AAJT in some future conflict settings where prolonged evacuation timelines could mean that complications outweigh potential benefit.
Limitations
The key limitation to synthesising the existing data, to report the effectiveness and safety of the AAJT-S, is a lack of high-grade evidence. This is compounded by the methodological heterogeneity between studies, and variability of outcome reporting. Limitations were also identified in the search strategy: not all relevant studies were identified with the original search criteria, but instead were found from full-text reference screening. This raises the possibility that not all relevant studies were identified.
Conclusion
There are limited data of safety and effectiveness of the AAJT-S. However, there is a requirement for a far-forward solution to improve NCTH outcomes, the AAJT-S is an attractive option and high-quality evidence is unlikely to be reported in the near future. Therefore, if this is implemented into clinical practice without a solid evidence base it will need a robust governance and surveillance process, similar to REBOA, with regular audit of use.
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
X @staceyjwebster, @edbarn
Contributors SW conceived the idea. SW, JER and EBGB undertook the systematic review, reviewed papers to determine inclusion and wrote and revised the manuscript. EBGB is responsible for the overall content as the guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.