Article Text

Abstract
Peripheral eosinophilia (>0.5×109/L) in the full blood count is caused by a variety of infectious and non-infectious aetiologies. Of particular importance to the UK military are parasitic infections, especially in individuals recruited from overseas and those who have deployed to areas that are highly endemic for schistosomiasis, strongyloidiasis and soil-transmitted helminths. These infections may persist for decades without causing symptoms. UK Armed Forces (UKAF) personnel have recently presented with more severe forms of strongyloidiasis, which can be fatal, especially following immunosuppression for chronic non-communicable diseases. Most uncomplicated infections respond to oral ivermectin or oral praziquantel, which are easy to take and generally well tolerated. We present the histories of three UKAF personnel to raise awareness of these infections, and we describe a framework for the initial investigation and management of people found to have eosinophilia in military primary care settings, together with indications for onward referral to infection or haematology specialists. Furthermore, given their relatively unknown prevalence in the UKAF Forces population, increased awareness and seroprevalence studies may be beneficial.
- Tropical medicine
- PARASITOLOGY
- Pathology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Eosinophilia is frequently encountered in military primary care. National guidelines for the management of eosinophilia in the general population exist, but military populations have differing demographics and risk factors for acquired eosinophilia.
Parasitic infections are the most common cause of eosinophilia in military populations, especially strongyloidiasis, schistosomiasis and soil-transmitted helminths. Recognition and investigation are important, as strongyloides infection is often asymptomatic but can be fatal if a patient subsequently becomes immunosuppressed.
WHAT THIS STUDY ADDS
This article provides a diagnostic framework for the initial investigation of eosinophilia for military primary care clinicians.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
This article should be used as a basis for military primary care clinicians to investigate eosinophilia.
Introduction
Peripheral blood eosinophilia is a common reason for referral to a haematology or infection specialist.1 2 Military personnel often travel to regions with endemic parasitic infections and can present with related eosinophilia.3 4 In addition, the UK Armed Forces (UKAF) recruit personnel widely from Commonwealth countries, where they may have acquired parasitic infections before joining the military.4–6 These infections are often asymptomatic or mild but can present with a myriad of symptoms to non-specialists, leading to diagnostic uncertainty.1
Eosinophils are tissue-dwelling leucocytes involved in host immune responses to infection, tissue remodelling, tumour surveillance and other immune functions.7 8 The normal peripheral blood eosinophil count is less than 0.5×109/L, with eosinophilia defined as levels above this.1 Table 1 lists some causes of eosinophilia.
Some causes of eosinophilia, listed within groups
We describe three cases, to illustrate how people with parasitic infections causing eosinophilia may present to a military clinician. This is followed by brief reviews of strongyloidiasis, schistosomiasis and soil-transmitted helminths; the most common parasitic causes of eosinophilia in military personnel, together with a framework to assist in initial diagnostic evaluation of eosinophilia.
Clinical cases
Case 1: coincidental finding of eosinophilia
A 37-year-old Fijian soldier presented with a fleeting skin rash, which the soldier described as raised. In the preceding 5 years, he had travelled to Bahrain, Belize, Kenya, the Falkland Islands and Fiji. Full blood count revealed an eosinophil count of 2.3×109/L. His travel history raised the suspicion that there may be a parasitic infection.
Serology and microscopy of a terminal urine sample were negative for schistosomiasis. Serology performed in primary care for Strongyloides stercoralis was positive (0.97 optical density (OD), upper limit of normal 0.20 OD). He was transferred to secondary care for outpatient treatment of presumed chronic strongyloidiasis with ivermectin. Repeat eosinophil count normalised (0.3×109/L) 6-months later.
Case 2: respiratory symptoms
A 28-year-old Fijian diver presented in the UK with a 1-year history of persistent dry cough at his annual diving medical. In the past 3 years, he had only travelled to the Falkland Islands and Fiji. A chest X-ray was normal but an obstructive pattern on spirometry (forced expiratory volume in 2 s (FEV1) of <80% of predicted normal and FEV1/forced vital capacity ratio of 0.62). Common lung pathologies and tuberculosis were excluded. In view of a peripheral eosinophil count of 1.1×109/L, S. stercoralis serology was performed and was positive (0.64 OD, upper limit of normal 0.2). He was treated with a single dose of ivermectin. 6 months later, his cough had resolved, his eosinophil count had fallen to 0.5×109/L and his Strongyloides serology had almost returned to normal (0.21 OD). His spirometry returned to normal and he was cleared for full diving duties.
Case 3: asymptomatic eosinophilia
A 35-year-old infantry soldier was found to have a high eosinophil count (1.2×109/L) during routine medical screening. He did not have any specific symptoms but disclosed significant freshwater exposure when on deployment to Kenya 3 years previously. Urine dipstick testing revealed microscopic haematuria. Subsequent investigations for schistosomiasis included positive serology for Schistosoma spp (titre 1:256) and a negative ultrasound scan of his renal tract. He was treated with oral praziquantel and followed up in clinic 6 months later, where his eosinophil count normalised (0.4×109/L) and haematuria had resolved.
Investigation of eosinophilia
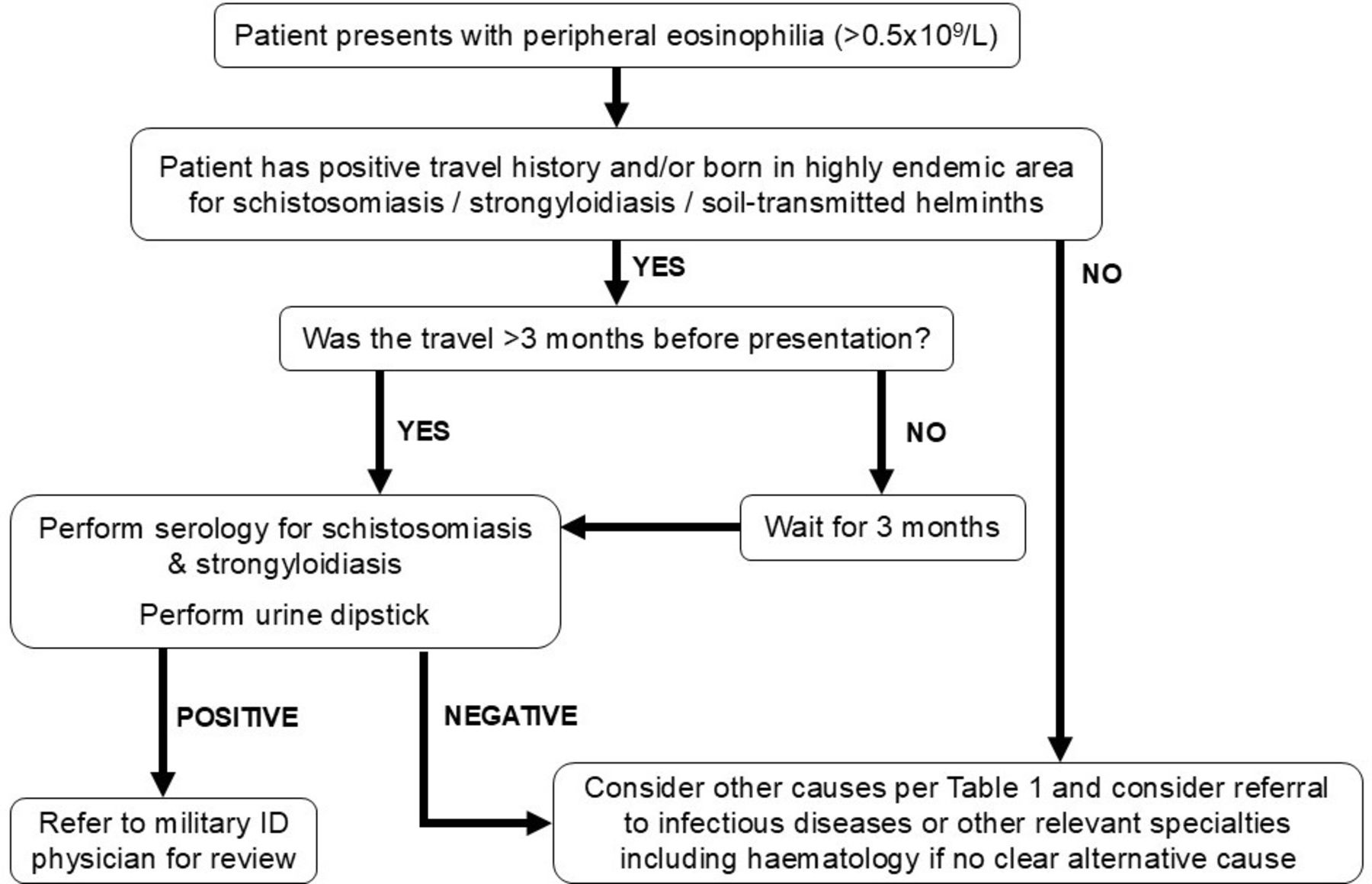
It is essential to take a thorough history including details of travel and exposures (animal, occupational, soil, water and diet), atopy and any recently started medications.1 Full examination of individuals should include special focus on the skin, the abdomen (especially for hepatomegaly and/or splenomegaly), the presence of lymphadenopathy and respiratory abnormalities.1 9 Patients may also have images on smartphones or other devices of transient skin signs that have resolved.10 Figure 1 shows a proposed algorithm for the investigation of eosinophilia in UKAF personnel.

Proposed algorithm for initial investigation and management of eosinophilia in individuals with a relevant travel history.
Strongyloidiasis
Strongyloidiasis is a parasitic infection that is usually caused by the nematode S. stercoralis, which can infect humans, other primates, cats and dogs.11 12 S. stercoralis is endemic in regions with poor sanitation, as well as foci in Southern Europe, the Southern USA and Japan.6 12 Larvae are excreted in the faeces of infected humans and animals and thrive in warm moist soil. Infection is predominantly by the transdermal route, following skin contact with larvae in contaminated soil.12 After tissue migration into the vasculature, the larvae migrate to the lungs, ascend the trachea, are expectorated, swallowed, before reaching the small bowel where they mature into adult worms, which release eggs into stool.12 Eggs hatch L1 larvae within the bowel lumen, which are excreted into soil to mature into infective L3 larvae. Some L1 larvae mature into L3 larvae within the host and penetrate the perirectal mucosa or perianal skin, starting an autoinfection cycle which can persist for decades.11 12 The symptoms of strongyloidiasis range from asymptomatic infection to chronic abdominal and respiratory symptoms (table 2).
Presentations of strongyloidiasis
In the immunocompetent host, chronic S. stercoralis infection is usually asymptomatic, but some individuals describe a pathognomonic ‘larva currens’ skin rash (figure 2). In the immunocompromised host, reduced immune control of autoinfection can lead to hyperinfection and disseminated infection (table 2).12 These hyperinfection states may occur many years after asymptomatic primary infection and are associated with a high mortality of up to 50%,13 due to overwhelming larval penetration, secondary Gram-negative bacteraemia and sepsis.14–16

Picture of cutaneous larva currens. Larva currens lesions are transient, rapidly moving pruritic linear streaks on the trunk, upper thighs, buttocks. With permission of Dr Geoff Gill and Prof Nicholas Beeching, Liverpool School of Tropical Medicine.
Factors associated with hyperinfection and disseminated infection include infection with human T- lymphotropic virus 1 and immunosuppressive medications, particularly corticosteroids, as well as alcohol abuse and organ transplantation.12
Incidental eosinophilia may be identified in people with asymptomatic infections, but eosinophilia is not a sensitive marker, being present in only around 75% of chronic infections in migrant populations and other groups with long-standing infection such as ex Far East Prisoners of War.17 18 In hyperinfection, eosinophilia is usually absent.12 In chronic infection, concentrated faecal microscopy usually has less than 30% success.12 Serological methods such as ELISA are both sensitive (84%–95%) and specific (>90%) in chronic infection19 but of limited value early in acute infection and hyperinfection.1 Other limitations of serological tests include cross-reactivity, especially in filarial and heavy hookworm infections. Ideally, patients should be followed up for at least 6 months to ensure resolution of any symptoms, eosinophilia or abnormal faecal tests; cure is often associated with a downward trend in serological titres, but serology may remain positive for several years after successful treatment and there is no uniform serological cut-off defining cure.12
The treatment of choice for uncomplicated (mild or asymptomatic) strongyloides infection is ivermectin orally 200mcg/kg/day STAT.20 Albendazole 400 mg orally twice daily for 7 days is an alternative but is less effective than ivermectin.21 The optimal treatment of hyperinfection syndrome includes reducing immunosuppression if safe and practicable, followed by daily ivermectin 200 μg/kg orally, subcutaneously or rectally, until stools are negative for 2 weeks.13
Schistosomiasis
Schistosomiasis is a chronic parasitic blood fluke infection acquired through contact with contaminated freshwater.22 The three major species of Schistosoma spp that cause human disease are Schistosoma mansoni (Africa and South America), Schistosoma haematobium (Africa and Middle East) and Schistosoma japonicum (East Asia).22 S. mansoni and S. japonicum cause predominantly gastrointestinal disease, whereas S. haematobium primarily causes genitourinary tract disease.22
Infection typically occurs when swimming or showering in freshwater containing the larval stages, called cercariae.22 These penetrate the skin and migrate to the liver via the circulation, subsequently maturing over a 2–4 weeks period. Once matured, the adult worms migrate to mesenteric venules of both the large and small bowel (S. japonicum), the mesenteric venules in the colon (S. mansoni) and the vesical venous plexus (S. haematobium).22 After several months, the female fluke starts to lay eggs, which are shed into the host urine or faeces. The migration of eggs through tissue causes chronic eosinophilic granulomatous reactions, resulting in tissue damage and scarring. Chronic inflammation in the bowel can lead to ulceration and bleeding; in the liver, periportal fibrosis leads to portal hypertension. Finally, within the urinary tract, the chronic granulomas can cause polyps which can transform into transitional cell carcinoma.21 Rarely the adult worms can migrate into the central nervous system, leading to egg deposition in the brain and spinal cord.21
Shortly after water exposure, an acute short-lived dermatitis (‘swimmer’s itch’) may occur at the site of cercarial skin penetration.22 Some individuals develop an acute schistosomiasis syndrome (‘Katayama fever’) which is a systemic hypersensitivity reaction to circulating Schistosoma spp antigens.21 Symptoms typically occur 2–8 weeks after water exposure but may commence earlier or later. They include urticaria, myalgia, arthralgia, dry cough, headache, fever, diarrhoea, abdominal pain, altered semen consistency and colour (sometimes with blood) and rarely, encephalitis.21 Peripheral eosinophil counts are typically raised (often very high) a few days after symptom onset.21
Eosinophilia is a common laboratory finding in up to 60% of individuals, especially in acute schistosomiasis.22 Anaemia can be observed in chronic disease, secondary to blood loss from the gastrointestinal or genitourinary tract. Urinary dipsticks are useful screening tests, especially in those with freshwater exposure in endemic regions.23 Light microscopy to detect eggs in faeces/urine is the current gold standard for confirming active infection. PCR and similar molecular methods are now in routine use in some laboratories and can offer increased sensitivity and practicality over concentration and microscopy, where multiple samples over multiple days must be obtained and processed. However, they still need more standardisation.24 Serology using ELISA or immunofluorescent antibody methods is usually positive within four to 8 weeks after exposure (sometimes up to 3 months) and is the most common method to diagnose chronic infection in the UK. However, serology can remain positive for years after successful treatment and cannot be used for test of cure.25
Delaying praziquantel for at least 8 weeks is advised for swimmer’s itch.22 In acute schistosomiasis syndrome (Katayama fever), treatment is with a single dose of praziquantel (40 mg/kg) on diagnosis, repeated in 8 weeks, with prednisolone 30 mg daily for at least 5 days.1 In chronic infection, the dose of praziquantel is 40 mg/kg once for all species except S. japonicum and S. mekongi which are treated with 60 mg/kg stat.22 Screening for Strongyloides should also occur.24
Soil-transmitted helminths (geohelminths)
In addition to strongyloidiasis, geohelminth infections include roundworms (ascariasis), hookworms and whipworms (trichuriasis), which are all common childhood infections throughout most of the tropics.1 Eosinophil counts may be substantially raised during early acute infections with these worms, but chronic infections may only be associated with slightly elevated or normal eosinophil counts. Acute infections can present gastrointestinal and dermatological complaints (figure 3), and eosinophilia as observed in numerous UKAF personnel following operations in Sierra Leone.3 Chronic geohelminth infections are usually asymptomatic and are typically detected by faecal microscopy performed as part of investigation for eosinophilia or following routine screening policies already in place for recruits from an endemic area.5

{kind=link}
{kind=link}
{kind=link}
Picture of cutaneous larva migrans. Itchy rash of cutaneous larva migrans caused by animal hookworm larvae, moving a few millimetres a day and lasting for weeks if untreated.
Discussion
Patients may present to UK military clinicians with eosinophilia. Parasitic causes should be high on the differential list, due to the recruitment of service personnel from and deployments to regions with a high helminth prevalence. Of these, both strongyloidiasis and schistosomiasis need to be diagnosed and treated, to prevent potentially serious complications. A detailed travel and exposure history is essential, and we commend the algorithm in figure 1 to aid initial investigation and possible subsequent referral.
The UKAF recruits personnel widely from Commonwealth countries. There has been a recent spike in the diagnosis of Fijian recruited personnel with acute and chronic strongyloidiasis. The Pacific Islands have not traditionally been recognised as highly endemic areas for S. stercoralis infection in occupational screening protocols, but there is increasing evidence for high regional levels of infection, which may exceed 30% in military personnel from Fiji.26
Routine screening for geohelminth infection is currently limited to specific foreign-born recruits and special forces personnel. Further work is required to investigate the prevalence of strongyloidiasis, schistosomiasis and geohelminth infections in UKAF personnel, especially in individuals recruited from Commonwealth countries and in those deploying to high-risk areas. This will inform the clinical need and cost effectiveness of targeted screening programmes of recruits and after different types of deployment and exercises.
Ethics statements
Patient consent for publication
References
Footnotes
MJWK, CH and WN are joint first authors.
X @nickbeeching, @NavyTropMed
Contributors MJWK, CH, WN and SW were responsible for the conceptualisation of the paper and composing the manuscript. CH and WN were responsible for reviewing the patients and obtaining consent. NJB and SW were responsible for supervising the drafting of the manuscript. MJWK, CH, WN, MKO'S, TF, SD, AC, MB, NJB and SW reviewed and revised the manuscript. SW is the guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.